Sparky
Well-Known Member
Thanking you in advance for your comments and suggestions. I really have to work on this area.......
17. Provide the CPT and ICD-9 diagnosis codes for the following scenario.
INDICATIONS: The patient had a YV advancement flap and advancement of the hamstring muscles about 3 weeks ago, but the wound separated and the muscles retracted over the area of the bone. She has had moderate separation of the wound but not complete separation, and we plan to minimally debride this area and resuture the wound with tension sutures.
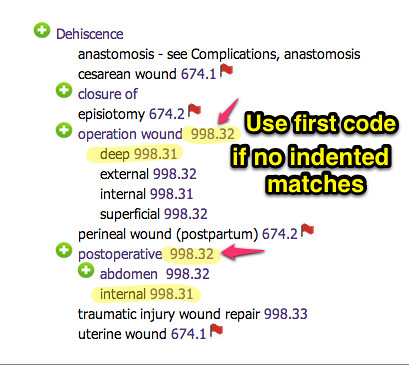
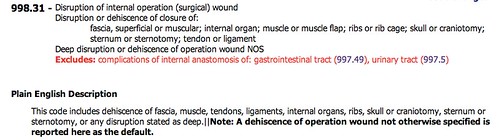
DIAGNOSIS: Wound dehiscence, left ischial area, partial.
SURGICAL FINDINGS: A 6 cm long by about 4 cm deep wound dehiscence.
PROCEDURE PERFORMED: Debridement of ischial wound by curettage with secondary wound closure.
PROCEDURE: The patient was intubated and turned in the prone position. The area was prepped with Betadine scrub and solution and draped in routine sterile fashion. The area was curettaged and a piece of the tissue was placed in a culture tube. This was curettaged down to bleeding granulation tissue. I was reluctant to restart by complete debridement of all these areas, because there are factors operative in this wound that are probably beyond our control. We nevertheless completed debridement of the granulation down to bleeding tissue and put far/near, near/far tension type sutures in the wound using #2 Ethibond. I then put some Xeroform underneath the sutures that were holding the wound together and put three boxes
of Kerlix Fluffs on top of this to cover some of the open areas on the thigh. The thigh sutures were also removed. I then taped the three boxes of Kerlix Fluffs to the ischial area with Elastoplast and taped around the leg to hold this in place, placing an ABD pad over the open areas where the sutures had been present. I then taped the buttock and leg up on the lumbar area with Elastoplast in such a manner as to support the ischial closure. A home health care nurse was in attendance at this time, and she was advised as to how to retape and dress this on a daily basis.
The patient had two open areas of the thigh and right lower leg, one of which was a donor site, the other of which was an old skin graft with open areas. We applied Scarlet Red and ABD pads to this area. Estimated blood loss 50 cc. Otherwise, the patient tolerated the procedure well and left the area in good condition.
Answer: CPT Code: 97602
Answer: ICD-9-CM Code: 998.31, 13160 (Comments: Incorrect code in red)
17. Provide the CPT and ICD-9 diagnosis codes for the following scenario.
INDICATIONS: The patient had a YV advancement flap and advancement of the hamstring muscles about 3 weeks ago, but the wound separated and the muscles retracted over the area of the bone. She has had moderate separation of the wound but not complete separation, and we plan to minimally debride this area and resuture the wound with tension sutures.
DIAGNOSIS: Wound dehiscence, left ischial area, partial.
SURGICAL FINDINGS: A 6 cm long by about 4 cm deep wound dehiscence.
PROCEDURE PERFORMED: Debridement of ischial wound by curettage with secondary wound closure.
PROCEDURE: The patient was intubated and turned in the prone position. The area was prepped with Betadine scrub and solution and draped in routine sterile fashion. The area was curettaged and a piece of the tissue was placed in a culture tube. This was curettaged down to bleeding granulation tissue. I was reluctant to restart by complete debridement of all these areas, because there are factors operative in this wound that are probably beyond our control. We nevertheless completed debridement of the granulation down to bleeding tissue and put far/near, near/far tension type sutures in the wound using #2 Ethibond. I then put some Xeroform underneath the sutures that were holding the wound together and put three boxes
of Kerlix Fluffs on top of this to cover some of the open areas on the thigh. The thigh sutures were also removed. I then taped the three boxes of Kerlix Fluffs to the ischial area with Elastoplast and taped around the leg to hold this in place, placing an ABD pad over the open areas where the sutures had been present. I then taped the buttock and leg up on the lumbar area with Elastoplast in such a manner as to support the ischial closure. A home health care nurse was in attendance at this time, and she was advised as to how to retape and dress this on a daily basis.
The patient had two open areas of the thigh and right lower leg, one of which was a donor site, the other of which was an old skin graft with open areas. We applied Scarlet Red and ABD pads to this area. Estimated blood loss 50 cc. Otherwise, the patient tolerated the procedure well and left the area in good condition.
Answer: CPT Code: 97602
Answer: ICD-9-CM Code: 998.31, 13160 (Comments: Incorrect code in red)

")